Chronic Hemorrhoids
Types of Hemorrhoids | Diagnosis | Treatment Options | FAQ
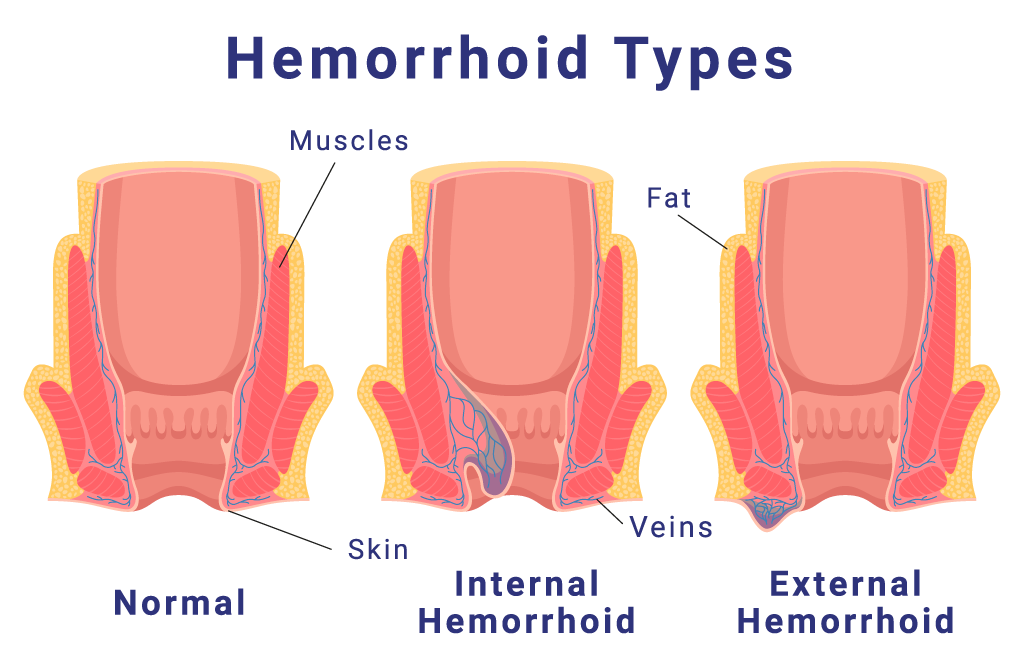
Approximately half of all Americans will experience hemorrhoids at some point. Also referred to as “piles” this condition causes veins around the anus and lower rectum to swell and become inflamed. They can be uncomfortable and itchy, and they cause bleeding during bowel movements. Most hemorrhoids will go away on their own, or with over-the-counter treatments at home. However, iIf hemorrhoids last longer than three months they are considered “chronic” hemorrhoids and may require treatment.
What causes chronic hemorrhoids?
Hemorrhoids can form for a number of reasons including straining during bowel movements, chronic constipation or diarrhea, lifting heavy objects, pregnancy, a low fiber diet, genetics, prolonged sitting, being overweight, anal fissures (small tears in the anus) and other factors. They are similar in nature to varicose veins.